Overview
Prostate cancer is the most commonly diagnosed cancer in men in Singapore. Prostate cancer can be slow-growing or aggressive. The aggressiveness of the cancer depends on the Gleason score. Cancers with Gleason scores of 6 and below are generally considered less aggressive, cancers with Gleason scores of 8 and above are considered very aggressive and cancers with Gleason scores of 7 are intermediate in terms of aggressiveness. Prostate cancer can be treated with minimally invasive methods.
Symptoms
Prostate cancer may not cause any symptoms in the early stage. Men may be diagnosed with prostate cancer as a result of health screening, or when they see a doctor for urinary symptoms such as:
– taking a long time to initiate urination
– slow urine stream
– interrupted urine stream
– inability to empty the bladder completely
– frequent urination
– frequent waking up at night to pass urine)
It is important to note that these symptoms can also be caused by non-cancerous enlargement of the prostate.
Advanced prostate cancer can cause other symptoms such as:
– passage of blood in the urine and semen
– back and hip pain (from spread of cancer to the bones)
– fatigue (from anaemia)
– leg swelling (from cancerous involvement of the pelvic lymph nodes and compression of the pelvic veins)
Diagnosis
There are two tests that are routinely performed to screen for prostate cancer:
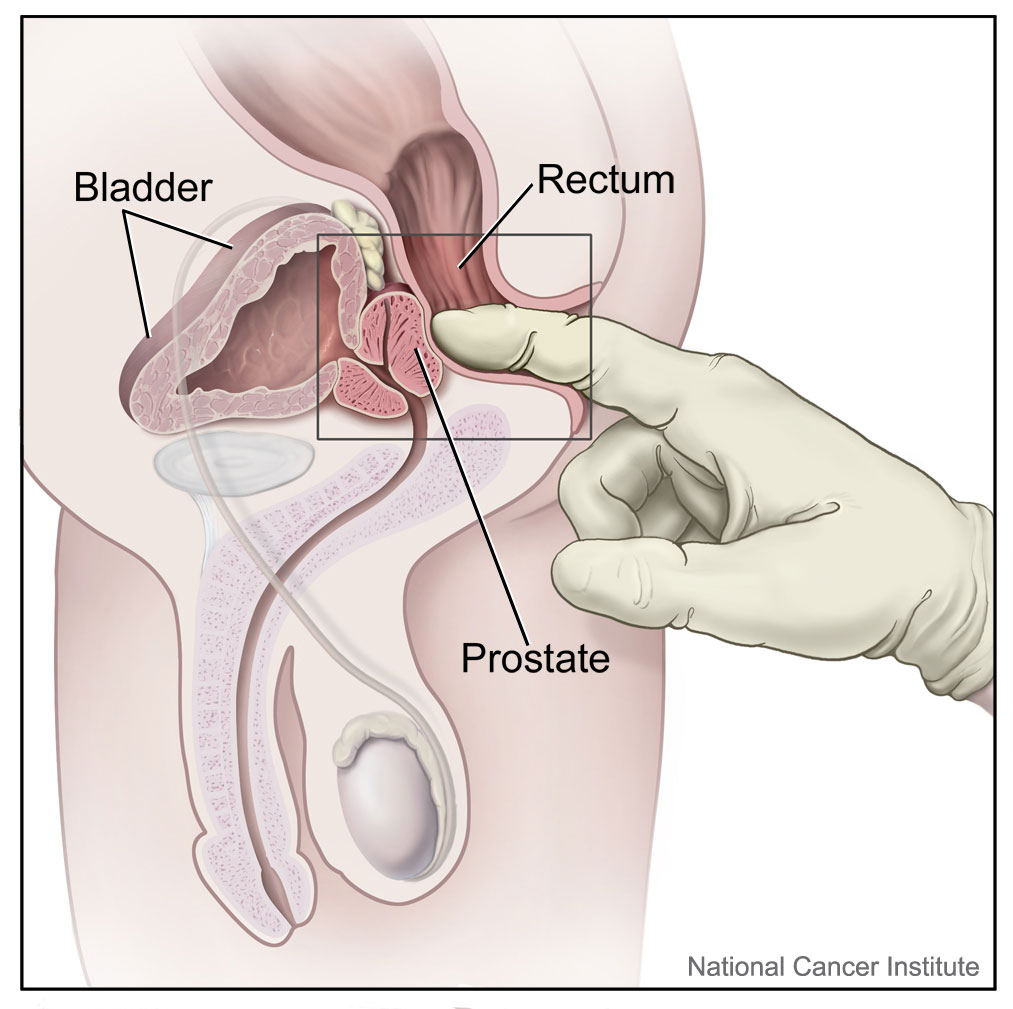
Rectal examination
The doctor will examine the prostate gland by gently inserting a gloved finger into the rectum. Prostate cancer can be suspected if the doctor feels a hard nodule within the prostate.
Serum PSA (prostate-specific antigen)
This is a blood test that gives an indication if there is cancer. An elevated level of PSA may indicate the presence of prostate cancer. However this test is not conclusive, and not all patients with elevated PSA levels have cancer; other diseases of the prostate such a benign prostatic enlargement and chronic inflammation (prostatitis) may cause abnormal PSA readings.
If either the rectal examination or the serum PSA are abnormal, the patient may be advised to undergo a prostate biopsy.
Transrectal ultrasound-guided prostate biopsy
This is usually performed in the office as a day procedure. It can be performed local anaesthesia or intravenous sedation. The patient lies on his right side with his legs brought up to his chest. An ultrasound probe is inserted gently into the rectum, a special channel attached to the probe allows passage of a small biopsy needle, through the rectal wall, into the prostate. With the biopsy needle, 10 to 12 cores of prostate tissue are obtained. Additional cores may be taken from areas that look suspicious on ultrasound or MRI. The tissue samples are then sent to the pathology laboratory for microscopic examination. The procedure takes about 10 minutes to perform.
Diagram below from Cancer Research UK
![]()
Transperineal ultrasound-guided prostate biopsy
Instead of performing the biopsy through the rectum, transperineal biopsy is a technique in which the biopsy needle is inserted through the perineum (the area between the scrotum and anus). This potentially reduces the risk of infection after biopsy.
Diagram below from Cancer Research UK
![]()
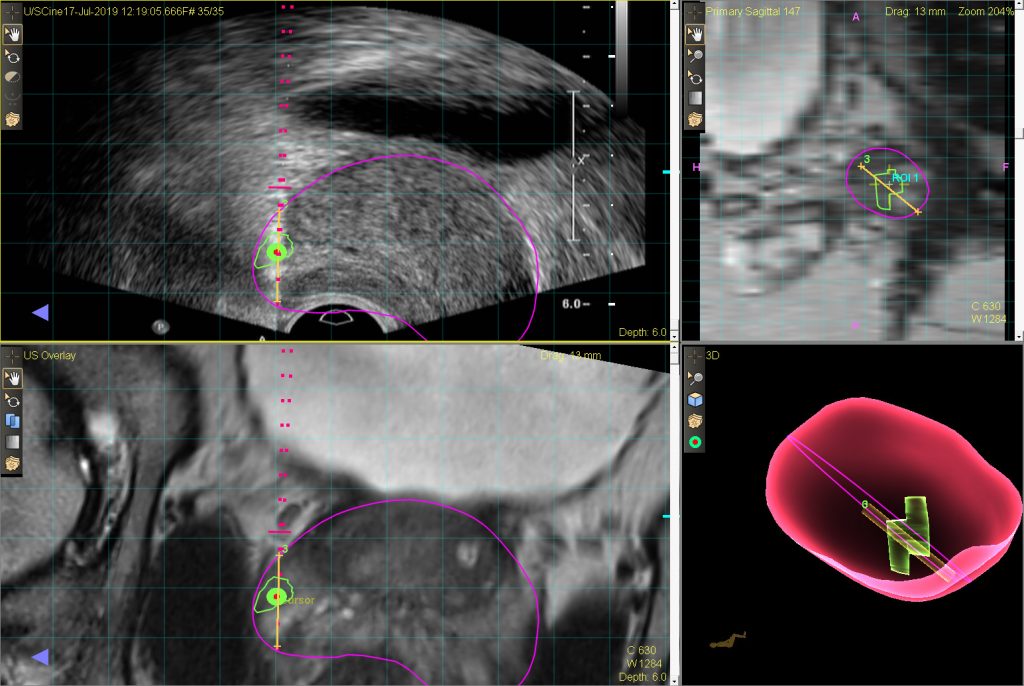
Targeted biopsy using MRI-ultrasound fusion
A new biopsy technique called MRI-ultrasound fusion guided biopsy of the prostate allows the prostate biopsy to be performed with more precision. Click on the link below to find out more.
Click on the following link to find out more about our prostate cancer screening package.
https://www.urospecialist.com.sg/article/prostate-cancer-screening/
Treatments
If the cancer is confined within the prostate, there are four main options – surgery, external beam radiotherapy, brachytherapy and active surveillance. Surgery, external beam radiotherapy and brachytherapy have the potential to cure the cancer . Active surveillance means that the patient is monitored closely without undergoing any treatment.
If the cancer has spread to the bones, lymph nodes or other organs (metastatic prostate cancer), hormonal therapy can be started to control the disease.
Active Surveillance
Patients with early low grade prostate cancer may live for many years before being affected by the disease. Bearing in mind that all prostate cancer treatments come with side-effects, these patients may choose not to go for treatment but instead opt to be closely monitored. This is termed as ‘active surveillance’. Patients should be monitored with regular PSA tests and repeat prostate biopsies. Patients can go for treatment if the cancer shows signs of progression.
Surgery (Radical Prostatectomy)
This is surgery to remove the prostate gland. The surgery is performed using open method through an incision in the lower abdomen (radical retropubic prostatectomy) or minimally invasive method (robot-assisted laparoscopic prostatectomy). The main advantage of robotic over open surgery is that the blood loss is usually less. During the first part of the surgery, the entire prostate is removed together with the seminal vesicles. Following that, the bladder neck is sutured back to the urethra. A urinary catheter is inserted to drain the bladder for one or two weeks. Usually the patient stays in hospital for 4 – 5 days.
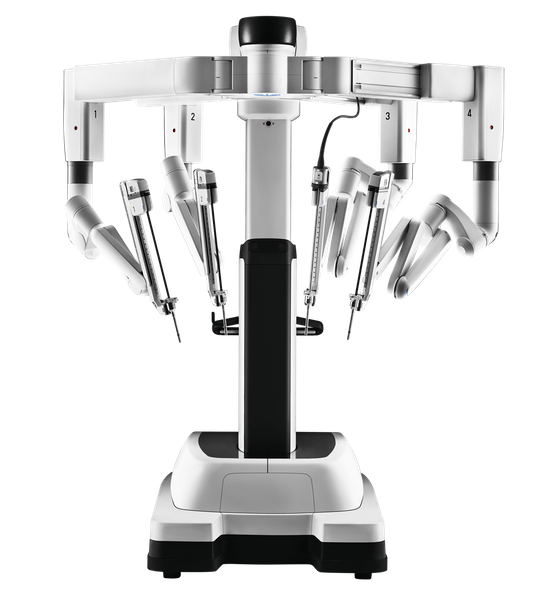
The Da Vinci robot used for robot-assisted laparoscopic prostatectomy (image from www.intuitive.com)
Advantages of surgery
The advantages of surgery are:
- High cure rate
- The patient has the assurance that the disease is removed from his body
What are the limitations of surgery?
If the cancer is confined to the prostate, surgery alone can provide a complete cure. If the cancer involves the edge of the prostate or beyond, patients may need to undergo radiotherapy or hormonal therapy after surgery.
What are the side-effects of surgery?
The main side-effects of radical prostatectomy are erectile dysfunction, stress urinary incontinence and occurrence of stricture (narrowing of the bladder neck). The control of urine usually gets better with time. Erectile dysfunction may improve with medication. Narrowing of the bladder neck may make it more difficult for the patient to urinate. These side effects may affect patients’ quality of life. There are treatments available to help with these side effects.
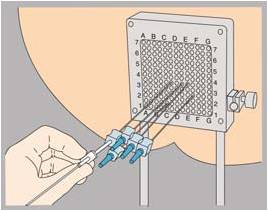
Brachytherapy for prostate cancer
Brachytherapy is a form of radiotherapy whereby the radioactive sources are directly inserted into the prostate rather than directed from an external source. The entire procedure is performed using needle punctures under general anaesthesia. Typically the patient is discharged on the evening of the procedure day, or the day after.
What are the advantages of brachytherapy?
The advantages of brachytherapy are:
- Short duration of treatment.
- Low surgical risk compared to radical prostatectomy
- Early recovery after procedure
What are the limitations of brachytherapy?
Brachytherapy is suitable for patients with ‘low-risk’ disease, ie. those with low stage and low grade prostate cancer. Some patients with ‘intermediate-risk’ disease with higher grade cancers can be considered for treatment as well.
It is not suitable for patients with ‘high-risk’ aggressive disease, or those with disease which is not confined to the prostate. Such patients are better treated with external beam radiotherapy or surgery.
What are the side-effects of brachytherapy?
Potential side-effects of brachytherapy include pain, urinary retention, increased urge to urinate and passage of loose stools. These side-effects are usually temporary and treatable with medication.
External beam radiotherapy
External beam radiotherapy is a form of treatment whereby radiation is focused onto the prostate from a source which is outside the body.

External beam radiotherapy machine (image from Narenfox)
What are the advantages of external beam radiotherapy?
The advantages of external beam radiotherapy are as follows:
- There is no anaesthesia or invasive procedure required. This procedure is suitable for patients who are old or have medical problems making them unfit for surgery.
- It can be used to treat cancers that have gone out beyond the confines of the prostate.
What are the limitations of external beam radiotherapy?
As there is a limit to the amount of radiation that can be given to the patient at one time, the entire course of treatment is spread over two months.
What are the side-effects of external beam radiotherapy?
External beam radiotherapy can cause side-effects similar to that of brachytherapy ie. urinary retention, increased urge to urinate and passage of loose stools. These side-effects are usually temporary and treatable with medication.
Which is the better treatment for prostate cancer, surgery or radiotherapy?
Do click on the link to find out more.
Hormonal therapy
In cases where the cancer is advanced and has already spread to the lymph nodes or other organs, there is usually no benefit from treating the cancer with surgery or radiotherapy. In such cases, hormonal therapy is the preferred treatment. Hormonal therapy works by cutting off the supply of the male hormone testosterone to the prostate. Most patients opt for hormonal treatment in the form of injections every 3 months, which will suppress the production of testosterone by the testicles.
![]()
Alternatively they can choose to go for surgery to remove their testicles.
What are the advantages of hormonal therapy?
Hormonal therapy is very effective for treatment of cancer symptoms such as pain and bleeding. It allows patients with advanced cancer to regain their quality of life.
What are the limitations of hormonal therapy?
Hormonal therapy controls the cancer but does not cure it. Injections should be continued indefinitely every three months. After a few years, the cancer may become resistant to the hormonal therapy, and the patient may require additional methods of treatment such as second-line medications or chemotherapy.
What are the side-effects of hormonal therapy?
Hormonal therapy does not have much immediate side-effect. However long-term treatment can result in tiredness, mood swings, weakening of the bones (osteoporosis) and weight gain.
New treatments for metastatic prostate cancer
Recent years have seen the introduction of drugs such as abiraterone and enzalutamide. They were initially used as second-line treatment for metastatic prostate cancer that has become resistant to standard hormonal therapy. Now it has become standard to use these drugs as first-line treatment of the disease. Click on the link below to find out more.
https://www.urospecialist.com.sg/article/a-new-era-in-the-treatment-of-metastatic-prostate-cancer/
New treatments for non-metastatic prostate cancer which is resistant to hormonal therapy
Drugs such as apalutamide, enzalutamide and darolutamide have been found to be effective in the treatment of patients with non-metastatic prostate cancer which has become resistant to hormonal therapy. Click on the link below to find out more.
Risk Factors
The following are risk factors for prostate cancer:
Age – The likelihood of having prostate cancer increases with age. In post-mortem studies, more than 30% of patients in their 70’s who died of unrelated conditions were found to have cancer in their prostate gland.
Race – African-american men have the highest risk of prostate cancer (176 per 100000 per year) , followed by Caucasian men (110 per 10000 per year). In contrast, the prostate cancer incidence in Asian countries is only 3 – 13 per 10000 per year.
Genetics – Men who have a family history of prostate cancer, or who carry certain gene mutations (eg. BRCA gene mutation), have a higher risk of developing prostate cancer than the normal population.
Diet – The link between obesity and prostate cancer is not proven. Nevertheless, obese men are more likely to have lower serum prostate-specific antigen (PSA) test readings, possibly leading to delayed diagnosis and treatment of prostate cancer. Also surgery in obese men is more difficult and obese men may have a higher risk of dying of prostate cancer. A diet high in animal fat and red meat may also predispose a person to prostate cancer.